Treatment
The treatment of choice for endometriosis is the combination of laser laparoscopic surgery and pharmaceutical administration. With the aid of CO2 laser and the use of SwiftLase, the sublimation of endometriotic sites of origin can be performed safely and accurately, whether these sites are small lesions of peritoneal endometriosis, extensive endometriosis or chocolate cysts. After the surgery, it is advisable to follow treatment with GnRH agonist analogues.
VIDEO: Endometriosis of the rectovaginal septum.
Surgical treatment of peritoneal, ovarian and rectovaginal septum endometriosis is usually combined with pharmaceutical administration. The aim of such treatment is to suspend the function of ectopic endometrial tissue and is usually achieved with the use of GnRH analogues (GnRHa).
Laser laparoscopic surgery
It is the ideal method of treatment for endometriosis. The accuracy of this method allows the selective distraction of the damage and it protects the neighbouring vital organs and the healthy ovarian tissue. Sublimation with SwiftLase is superior to cauterization with the use of conventional electrosurgical units (diathermies), since just with the addition of SwiftLase we can achieve a small depth of sublimation in the tissue, which is known and specified from histological studies and does not leave any traces of carbon.
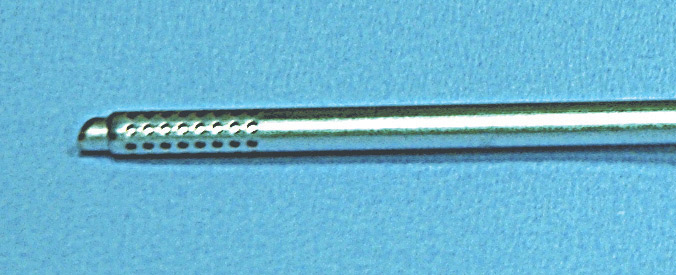
SwiftLase is a laser flash-scanner that is made up of two almost parallel mirrors that rotate fast with the aid of a special motor, which results in the fast movement of the focused spot size of the CO2 laser beam. Histological studies (Donnez et al., 1994) have proven that with the use of SwiftLase and laser with a power greater than 30 W, we can achieve surface sublimation of any damage without any traces of carbon. The crater that results in a 0.1 second has a 2.5 mm diameter and a 0.2 mm depth. Fine and slow movements along the observed damage with the laparoscope have a surgical treatment result of sublimation with a final depth of 0.05-0.1 mm.
Sublimation of peritoneal endometriosis with SwiftLase (laparoscopic image).
The aim of laser laparoscopic surgery in endometriosis is the lysis of any adhesions, the restoration of the normal anatomical relations, as well as the sublimation or the ablation of all visible endometriotic sites of origin. The use of laser CO2 with the addition of SwiftLase allows the sublimation of areas of peritoneal endometriosis that are located next to vital organs (urinary bladder, intestine, large blood vessels etc.). Moreover, retroperitoneal injection of saline allows the complete sublimation of any damage with safety.
Surgical reparation is hard and it includes, separation of the anterior wall of the intestine from the posterior wall of the vagina and the uterus and the removal of the adenomyotic nodule and the sublimation of any visible endometriotic lesion.
Surgical techniques
Small site on the surface of the ovary (<1cm diameter) can be treated easily with sublimation using SwiftLase.
Sublimation of a small ovarian endometrioma (EUGONIA archive).
For ovarian endometriomas (diameter <3cm) a small opening of 5 mm length is createdusing laser CO2 on the top of the cyst, the chocolate fluid is aspirated and the interior of the cyst is washed thoroughly with saline. After washing, the inside of the cyst is examined to confirm the absence of any suspicious stems on the interior (to exclude malignancy). If there is even a small suspicion, sublimation is not performed but a biopsy is taken.
If the interior is free of damages, sublimation at high power is performed. In this way only the ectopic endometriotic epithelium is destroyed, maintaining the underlying healthy ovarian tissue. The ovaries are then thoroughly washed.
Sublimation or removal of the cysts
Sublimation of ovarian endometrioma. The cyst has been incised and is sublimated with SwiftLase. (laparoscopic image).
The surgical practice of sublimation versus excision is the correct treatment choice, especially for endometriomas smaller than 3 cm. According to the classification of Nezhat (1995), they are regarded as true endometriomas, which are impossible to remove, because there is not an anatomical or histological separation plane of the endometrioma from the underlying ovarian tissue. According to the hypothesis of Hugheston (1957), ovarian endometriomas are the result of engulfment of surface fragments of endometriotic tissue in the ovary. Therefore, in the attempt of their removal based on an artificial separation plane between endometrioma and ovarian tissue, some ovarian cortex (containing follicles) is also removed. Sublimation of endometriotic cysts using Swiftlase has advantages over laparoscopic cyst removal, because after treatment ovarian reserve is maintained.
Sublimation of ovarian endometrioma. Detail of sublimation (laparoscopic image).
For endometriomas larger than 3 cm, after their opening, washing and examination to exclude any suspicious damage, follows careful peeling of the cyst from the ovarian tissue. If peeling is easy, the cyst is removed entirely. If there is strong adhesion then Swiftlase is used. In case that some sites of the wall are attached to the ovarian tissue, the cyst is partially removed and the remaining is sublmimated using Swiftlase.























 of uterine myoma laparoscopically with the use of CO2 laser")


















































